A moderate to severe PIP flexion contracture is difficult to treat with conventional hand therapy splints. The primary reason for splint failure is the amount of pressure they apply to the skin in their efforts to extend the joint. Brand and Hollister1 found that pressure on the skin during splinting should not exceed 50 gm/cm2 if the splint is to be worn for more than 8 hours at a time. Fess2 evaluated four different varieties of commercially available PIP extension splints and found that all of them generate a progressively higher force as the deformity increases. This force is transmitted via pressure on the skin of the finger. Consequently, long standing PIP flexion contractures or those contractures of more than 30-45 degrees cannot be effectively treated with dynamic PIP extension splints3.
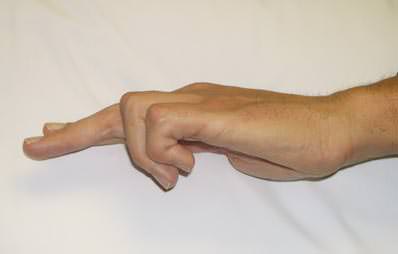
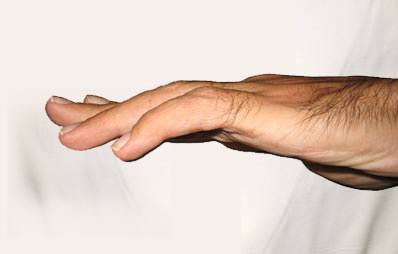
The Digit Widget avoids the skin pressure problems associated with conventional splinting by transmitting an extension torque directly to the joint by skeletal pins rather than through the skin, slowly reversing the contracture. If serial plaster casts or splints have failed, consider using the Digit Widget.
Single stage surgical release of a PIP contracture is also problematic. It must be remembered that the joint is not simply flexed. All of the soft tissues on the palmar side of the joint are shortened. Blood vessels and nerves may be compromised with sudden contracture reversal. Several studies have shown that the more structures released to gain PIP extension, the worse the final outcome4-7.
The Digit Widget is an effective tool in the treatment of moderate to severe PIP flexion contractures because it is able to extend a contracted PIP joint without surgical release of the volar structures, if the tissues are compliant and the joint is intact. The contracted tissues, rather than being surgically cut, are stimulated to lengthen over time.
As effective as the Digit Widget is in improving joint extension, in most cases it is not the only intervention needed. The questions below are a starting point in the patients’ evaluation. The surgeon must determine if the underlying cause of the contracture can be successfully treated and, if so, formulate a plan to rebalance the flexor and extensor forces.
- Is the cartilage space substantially normal?
- Is the central slip intact?
- Do x-rays show concentric alignment of the joint?
- Is the joint capable of gliding motion?
- Is normal length and alignment of the proximal phalanx present?
- Are the palmar tissues simply shortened or is there scarring from previous surgery or injury?
- Are adhesions between the extensor tendon and the proximal phalanx preventing active joint extension?
- Are adhesions or other mechanical obstructions preventing distal gliding of the flexor tendons?
- Are the flexor tendons bowstringing across the PIP joint?
- Is spasticity present in the flexor muscles?
- Are the intrinsic muscles weak or paralyzed?
References:
- Brand PW, Hollister AM: Clinical Mechanics of the Hand (3rd ed). St. Louis, Mosby, 1999, pp 218-219.
- Fess EE: Force magnitude of commercial spring-coil and spring-wire splints designed to extend the proximal interphalangeal joint. J Hand Ther Jan-Mar:86-90, 1988.
- Colditz, JC: Efficient mechanics of pip mobilisation splinting. Brit J Hand Ther 5:65-71, 2000.
- Curtis RM: Capsulectomy of the interphalangeal joints of the fingers. J Bone Joint Surg 36A:1219-1232, 1954.
- Curtis RM: Management of the stiff proximal interphalangeal joint. Hand 1:32-37, 1969.
- Ghidella SD, Segalman KA, Murphey MS: Long-term results of surgical management of proximal interphalangeal joint contracture. J Hand Surg 27A:799-805, 2002.
- Craft RO, Smith AA, Coakley B, Casey WJ, Rebecca AM, Duncan SFM: Preliminary soft-tissue distraction versus checkrein ligament release after fasciectomy in the treatment of dupuytren’s proximal interphalangeal joint contractures. Plast Reconstr Surg 128:1107-1113, 2011.